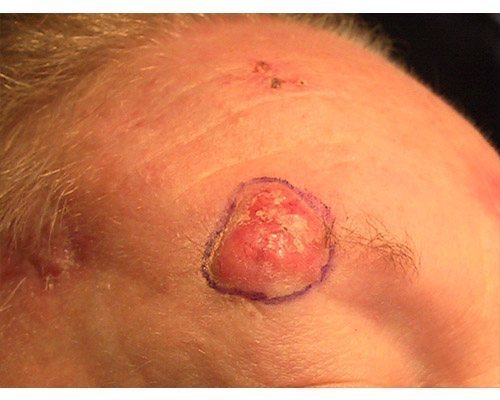
 A superficial basal cell carcinoma (BCC). Clinically, an erythematous, well-circumscribed macule with minimal scale is present. This tumor is often misdiagnosed as eczematous dermatitis or guttate psoriasis and is often difficult to distinguish clinically from Bowen disease (squamous cell carcinoma in situ). Features that suggest the diagnosis of superficial BCC are the absence of significant white, adherent scale, and a history of the lesion remaining unchanged for several months or years. Treatment options for this tumor include electrodesiccation and curettage, surgical excision, cryosurgery, 5-fluorouracil, 5% imiquimod cream, and superficial radiographic therapy. Electrodesiccation and curettage is the modality most commonly used, with a cure rate of approximately 95%. Basal cell carcinoma. Basal cell carcinoma. A 68-year-old patient presenting with an advanced A 68-year-old patient presenting with an advanced basal cell carcinoma (BCC) of the right periorbital region, frontal view (Images courtesy of M Abraham Kuriakose, DDS, MD)
A superficial basal cell carcinoma (BCC). Clinically, an erythematous, well-circumscribed macule with minimal scale is present. This tumor is often misdiagnosed as eczematous dermatitis or guttate psoriasis and is often difficult to distinguish clinically from Bowen disease (squamous cell carcinoma in situ). Features that suggest the diagnosis of superficial BCC are the absence of significant white, adherent scale, and a history of the lesion remaining unchanged for several months or years. Treatment options for this tumor include electrodesiccation and curettage, surgical excision, cryosurgery, 5-fluorouracil, 5% imiquimod cream, and superficial radiographic therapy. Electrodesiccation and curettage is the modality most commonly used, with a cure rate of approximately 95%. Basal cell carcinoma. Basal cell carcinoma. A 68-year-old patient presenting with an advanced A 68-year-old patient presenting with an advanced basal cell carcinoma (BCC) of the right periorbital region, frontal view (Images courtesy of M Abraham Kuriakose, DDS, MD)
BCC is a nonmelanocytic skin cancer (ie, an epithelial tumor) that arises from basal cells, which are small round cells found in the lower layer of the epidermis. Basal cells invade the dermis but seldom invade other parts of the body. The deoxyribonucleic acid (DNA) of certain genes is often damaged in patients with BCC; therefore, inheritance may be a factor. Most DNA alterations result from damage caused by exposure to sunlight. (See Pathophysiology.)
Body distribution of BCCs is as follows:
On the head (most frequently on the face; most common location is the nose, specifically the nasal tip and alae) – 70% On the trunk- 25% On the penis,vulva, or perianal skin – 5%







The anatomic distribution of BCCs correlates with embryonic fusion planes. Recent data indicate that after adjusting for surface area, BCC occurrence is greater than 4 times more likely on embryonic fusion planes than on other regions of the midface, a finding that supports the possibility of an embryologic role for BCC pathogenesis.
BCC can develop on unexposed areas, and cases of BCC of the prostate have been reported. In some patients, contributing factors are exposure to or contact with arsenic, tar, coal, paraffin,certain types of industrial oil, and radiation. BCC can also be associated with scars (eg, burn complications),xeroderma pigmentosum, previous trauma.vaccinations, or even tattoos. (See Etiology.)
A skin biopsy (most often a shave biopsy is sufficient) may be necessary to confirm the diagnosis and is often required to determine the histologic subtype of BCC. A punch biopsy may be used to obtain a thick specimen, especially when the clinical suspicion of a BCC is still present after shave biopsy results are negative. (See Workup.)
Neglected tumors can continue to grow and lead to significant local destruction and even disfigurement. Surgery, in almost all cases, is the recommended treatment, with treatments varying on the basis of cancer size, depth, and location. (See Treatment and Management.)
Superficial BCCS have been successfully treated with imiquimod 5% cream, and topical 5-fluorouracil 5% cream may be used to treat small, superficial BCCs. Several studies have shown success in treating small nodular BCCs with imiquimod 5% cream, although this is an off-label indication and patients should be informed of this fact. (See Medication.) Anatomy
Basal cell carcinomas (BCCs) occur predominantly on the head, with 70% of BCCs occurring on the head (most frequently on the face), 25% on the trunk, and 5% on the penis, vulva,or perianal skin. Very rarely, other organs are affected.
